
It’s no secret that OTs address bathing skills *insert sarcastic smirk here*. That being said, it’s one thing to provide ADL retraining to someone who has strong cognitive skills and understands their need to re-learn these skills. It is an entirely different thing to provide ADL retraining to someone whose cognitive skills are impacted and who may not fully understand their need for self care intervention.
So let’s talk about that.
First and foremost, we as the therapist have to fully know and understand what aspects of the task need work. Yet another reason why a comprehensive evaluation is so essential. (If you need to start there, I’ve got a Free Eval Kit just for you!)
From there, we get into the knitty gritty.
I like to start at a setup/supervision level.
Let me explain. I find that 9 times out of 10, if I allow someone to perform as much of the task as they can on their own (without me directly intervening) they’ll do more of the task than they would if I asked “Can you wash your face now?”.
So I’ll head into the bathroom with the patient and say something like “I’m just going to make sure you have everything you need”. Then I’ll get the water started, lather up a washcloth, and hand it to the patient. I might say “This is for your *insert body part here*” just to get the ball rolling. Then I’ll just hang back and watch. If I notice things are slow going, the patient isn’t initiating, or the patient is perseverating on just their arms and not moving to the rest of the body, I’ll say “If you need help let me know”. If the patient asks for help or the previously mentioned behaviors continue, then I’ll intervene. First with a visual and verbal cue, then with physical assist.
I’m not scared of external memory devices.
If I’m being honest, these were hard for me to get into. A checklist of steps listing each part of the body felt a little insulting at first. I was afraid that a patient would accuse me of thinking that they’re stupid or incompetent. And some patients are apprehensive at first.
But the honest truth: there’s usually notable improvement in sequencing and thoroughness when a checklist is placed in the bathroom. Repetition and consistency is key for individuals living with dementia. It’s in these spaces that neuroplasticity surprises us for the best.
Plus this is a great tool that can be taken home if that’s the plan for discharge or that can be integrated into the ongoing care plan on a long-term unit.
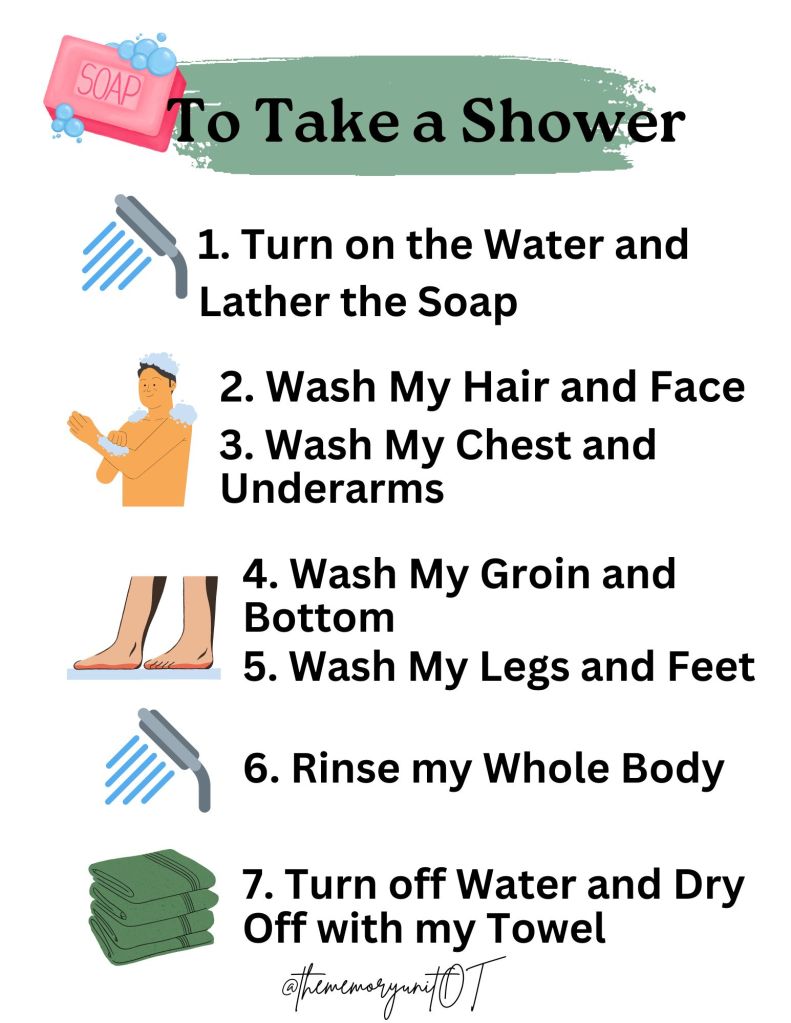
This is a very basic external memory aid that you’re welcome to print and use. I highly recommend tailoring this to be a bit more specific to the patient you’re treating, but hopefully this will give you a starting place!
Bathing interventions don’t only happen in the bathroom or shower.
We have to address all of the cognitive and biomechanical aspects of the task. A patient will never improve in lower body bathing if they can’t flex their hips past 90 degrees. They can’t properly wash their perineum if they can’t let go of the grab bar in standing or weight shift in sitting. They can’t get in and out of the tub if they never work on transfers or high steps. They won’t be able to tolerate the full shower if they’re short of breath after 1 minute of activity. They will never be able to recall the steps of the task if they’re never given the opportunity.
So I work on balance, stretching, strengthening, weight shifting, transfers, endurance, cardiopulmonary function, and cognition. All outside of their morning routine. Adaptive equipment can help, but why not improve in flexibility and strength first?
I have to strive for progress each week.
If I’m always providing the same levels of assistance, the patient will never meet their self care goals. We have to be confident in the interventions we provide. If a patient is actively improving in their strength, balance, and activity tolerance, I have to let them try within their self care routines.
And this can absolutely look like small steps. Inching from max assistance to mod to min. But you as the therapist have to be the one to initiate these progressions. It’s okay if it takes the patient a full 45 minutes to take a shower. Give them the time and the space to improve.
When we promote independence, despite stereotypes of age and ability, the results are surprisingly positive.







Leave a comment