A Patient-Specific Continence Management Program is essentially a fancy and professional-sounding way to identify and implement strategies that maximize your Patient’s ability to maintain continence. It is not a cookie-cutter exercise routine or schedule, but rather a program that you and your Patient create based on his or her specific needs and deficits.
Start the Conversation
Starting the conversation will identify the ‘why’ behind the need for a continence program.
Is this change in continence new? Can the individual always feel the sense or urge to go? Can the individual hold their urine until they reach the bathroom? Are episodes of incontinence becoming more frequent? Does the individual require external devices that were not previously used (pads, briefs, etc)? Is there a memory or cognitive impairment that impacts safe and thorough toilet use? Is there a physical impairment that limits safety with transfers or standing tasks in the bathroom? Does the individual require more assistance from family or staff to safely use the bathroom? Is this individual a candidate for pelvic floor strengthening? What supports will this individual have at discharge?
This looks and feels a lot like a formal evaluation, because that’s exactly what it is. And a full evaluation/assessment is the crucial first step in implementing a successful program.
Now I know this sort of conversation can feel a bit intimidating, especially if you don’t have a ton of experience yet. These are very personal issues that can feel awkward to talk about. But when approached empathetically and professionally, they can be highly successful. And for most individuals who are aware of and can advocate for themselves, they’re going to welcome the conversation because they likely want a solution.
Now because we primarily talk about Memory Care here, it’s important to note that this step still applies when creating a program for individuals living with dementia. While some Residents cannot reliably describe what they’re feeling and experiencing 100% of the time, these questions still need to be asked of both the Resident and the primary caregivers.
Gather the Data
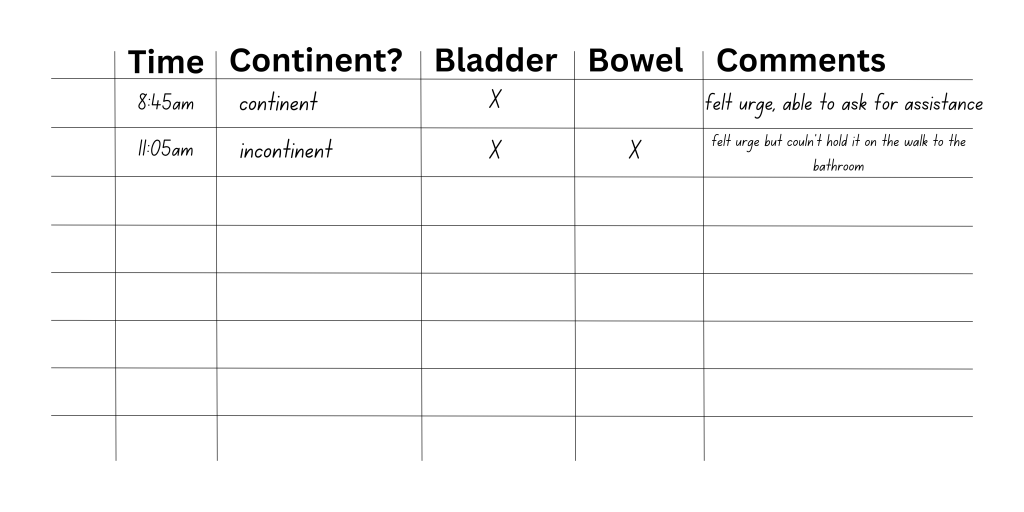
We’re talking about firm, objective data here. I like to use a basic chart for this step, collecting data over the course of several days. Each time the individual either uses the bathroom or experiences an incontinent episode, it’s documented. I make sure that I include whether or not the individual could feel the urge or sensation prior to the episode.
This is a crucial step in that evaluation and assessment process we just looked at. Even if your Patient or Resident is a strong historian and self-advocate, when an issue such as changes in continence has been ongoing, it can be hard to fully report every detail and routine in just one conversation.
So we essentially keep a journal of symptoms, to ensure that ALL areas and aspects are assessed and then addressed.
Identify the Trends & Patterns
Once you have the data collected, you’ll start to notice trends and patterns. I often find that episodes of incontinence occur the most within 1-2 hours after a meal, first thing in the morning, or during the night. I’ve even had one instance where we noticed a lactose sensitivity in a Resident because they were always incontinent of bowel after eating cold cereal and coffee with cream every morning for breakfast.
You just never know what you’re going to find, but this data will guide your next steps in developing the program.
Be sure to review these findings with the Patient and/or their family or caregiver to keep the patient-unit involved in the entire treatment planning process.
Trial the Strategies
From here, we’re going to trial different strategies. This could include pelvic floor strengthening, core strengthening, using the bathroom 10 or so minutes before an incontinent episode typically occurs (based on the data you collected), or automatically using the bathroom every 2-3 hours during the day and every 4-6 hours at night.
If it’s warranted to trial a toileting schedule, you as the therapist may need to provide it’s execution in the initial stages. In the long-term care setting, sometimes I’ll break my sessions up into 4 or 5 15-minute intervals. I will prompt the Resident to transition into the bathroom, and I will assist the Resident as needed. Once we’ve got an effective schedule and routine in place, I’ll then begin the process of either addressing the Resident’s independence with the schedule or training the care staff as needed.
Remember that this is not a one-size-fits-all prescription. And you may have to trial various combinations of strategies before you find the sweet spot that works the best for your Patient.
Address the Skills
We cannot neglect the physical and cognitive skills needed to effectively and safely use the bathroom. We have to consider balance (in sitting and standing), range of motion, strength, activity tolerance, cardiopulmonary function, equipment management, and transfer/mobility status along with perineal hygiene and strength. So use your sessions effectively. You don’t have to only focus on pelvic floor strength or execution of a toileting schedule. You can and should incorporate balance, strength, and endurance training as indicated and implement cognitive training and strategies as needed.
Train the Other Key Players
Once you have all the pieces and parts in place, you’ve got a schedule that works, and you’ve addressed the necessary skills, then you can begin training the Resident’s family or care staff in the program’s execution. I will typically include a long-term goal in my care plan that speaks directly to Caregiver training and carryover. This empowers me as the therapist to walk away after discharge knowing that I’ve done all I can do to maximize carryover beyond therapy intervention as much as possible.







Leave a comment