
Cooking tasks and groups are one of my favorite things to utilize in therapeutic sessions. It is especially helpful when addressing cognition, because there is so much involved in the process of planning and preparing a dish or dessert. Cooking and baking also incorporate several gross motor elements that allow us to address standing tolerance, balance, and functional reach while maintaining and individuals attention.
I like to start a cooking task or session by making a basic shopping list.
I’ll prompt the Resident by saying something like “I was thinking, let’s make some mini pizzas for lunch today. What ingredients do you usually use when you make a pizza?”
Of course, I already know the ingredients we’ll be using for the activity. But I like using this as a means of starting a conversation that requires memory, critical thinking, and executive function.
I’ve included a printable Shopping List here:

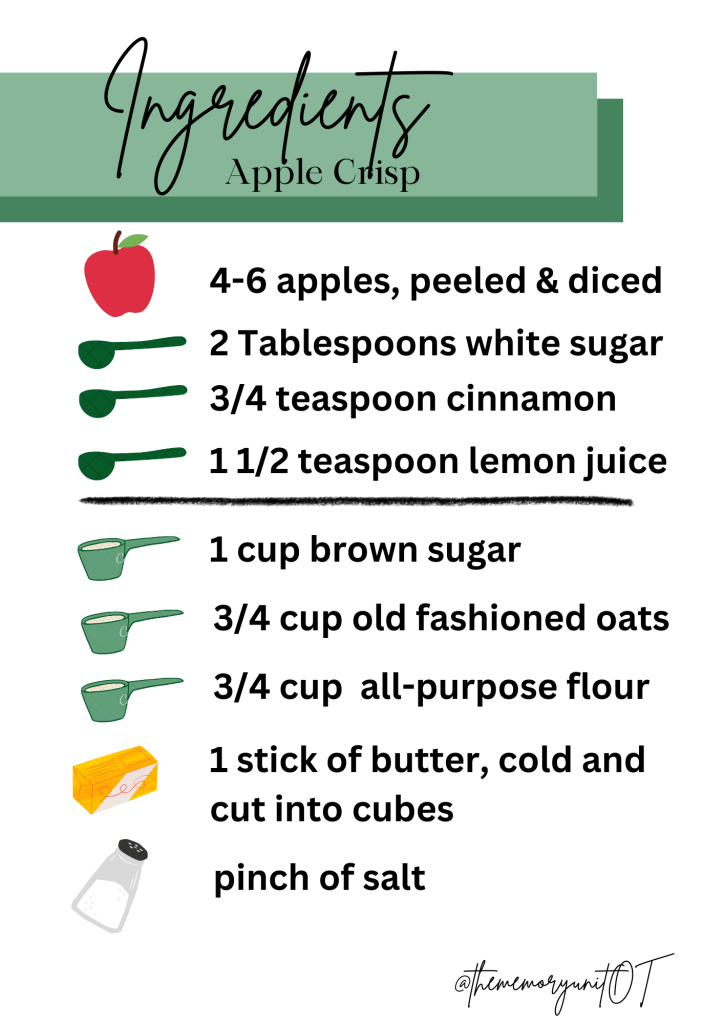
Apple crisp is such a classic fall treat. And usually at this point, you’ve got an abundance of apples that need to get cooked or eaten quickly.

This recipe calls for:
- 4-6 apples, peeled and then either chopped or sliced
- 2 Tbs granulated sugar
- 1 3/4 tsp ground cinnamon (divided)
- 1 1/2 tsp lemon juice
- 1 cup light brown sugar
- 3/4 cup old fashioned oats
- 3/4 cup all purpose flour
- 1 stick of butter, cold and diced into cubes
- pinch of salt
I’ve included an illustrated list of the ingredients that may be helpful for your Residents to better understand the measurements.
From here, we can start actually baking.
To make the crisp:
- combine apples, granulated sugar, 3/4 tsp ground cinnamon, and lemon juice in a large bowl
- transfer the apple mixture into a buttered 8×8 baking dish
- in a separate bowl, use a pastry cutter to combine brown sugar, oats, flour, 1 tsp ground cinnamon, salt, and butter
- spread topping mixture over apples
- bake at 350F for 40-50 minutes
I’ve again included an illustrated instruction sheet to act as a visual cue.

How to Bill for This Activity when Working with Someone Living in the Mild Stages of the Disease.
If you’re using this on The Memory Unit or Long-term Care Unit, the focus will likely be on the cognitive components of the task. But you can just as easily include balance, standing, reaching, and strength to the task by doing it in standing, placing the ingredients and utensils out of reach, adding a balance pad, or donning weighted wrist cuffs.
Your documentation should include things like:
- how many ingredients they could independently add to the shopping list
- the amount of assistance required to follow the directions
- the amount of errors made
- any safety cues that were required
- their overall tolerance of the task
- the physical position the individual performed the task in (sitting vs. standing)
- the amount of rest breaks provided
- and any other physical objective measures (such as vital signs, balance grade, or amount of weight added/used)
For individuals living with Mild Cognitive Impairment, or in the early stages of dementia, I honestly let them engage in most of the task. They use the utensils, they get involved in using the oven, and they help clean the dishes following the task. This is especially important if the individual is a short-term Client who will be returning home to live in the community.
It may feel ‘unsafe’ to have them use the oven…. but what are the chances they’ll use the oven at home? Probably pretty high. So we have to work on these skills within the parameters of therapy sessions.
How to Bill for this Activity when Working with Someone Living in the Moderate Stages of the Disease.
While the focus will still be on the cognitive components, the chances of this individual needing to independently and safely perform this sort of task at discharge are pretty low. Which means the cognitive emphasis is placed more on engagement and sequencing skills.
Because of this, your documentation should include things like:
- how long the Resident could tolerate the task
- how much physical assistance was provided
- the level of direction provided (single-step, multi-step, etc)
- the type of cues provided (visual, verbal, tactile)
- how many times the Resident required redirection
- the Resident’s emotional state throughout the task
For me, I’m using this type of activity to help someone living in those moderate stages more actively engage in a structured and meaningful task. It’s about maximizing their ability to participate in normal human tasks despite the presence of their disease.
related posts








{kind=link}
Leave a reply to It’s Almost Thanksgiving: Here’s How to Celebrate on The Memory Unit – The Memory Unit OT Cancel reply